
Lymphocytes
Share
Follow Us
Lymphocytosis is seen in infectious mononucleosis, viral hepatitis, cytomegalovirus infection, other viral infections, pertussis, toxoplasmosis, brucellosis, TB, syphilis, lymphocytic leukemias, and lead, carbon disulfide, tetrachloroethane, and arsenical poisonings. A mature lymphocyte count >7,000/µL is an individual over 50 years of age is highly suggestive of chronic lymphocytic leukemia (CLL). Drugs increasing the lymphocyte count include aminosalicyclic acid, griseofulvin, haloperidol, levodopa, niacinamide, phenytoin, and mephenytoin.
Lymphopenia is characteristic of AIDS. It is also seen in acute infections, Hodgkin’s disease, systemic lupus, renal failure, carcinomatosis, and with administration of corticosteroids, lithium, mechlorethamine, methysergide, niacin, and ionizing irradiation. Of all hematopoietic cells lymphocytes are the most sensitive to whole-body irradiation, and their count is the first to fall in radiation sickness.
About Lymphocytes:
In the immune/inflammatory response, if the neutrophils and monocytes are the brutes, the lymphocytes are the brains. It is possible to observe the horror of life without lymphocyte function by studying the unfortunate few with hereditary, X-linked, severe combined immune deficiency. Such individuals uniformly die of systemic infections at an early age (except for the “bubble boys” of yesteryear, who lived out their short lives in antiseptic prisons). The functions of lymphocytes are so diverse and complex that they are beyond the scope of this text (and the scope of the author, it must be admitted). What follows are a few general remarks concerning examination of lymphocytes in peripheral blood.
After neutrophils, lymphocytes are the most numerous of the circulating leukocytes. The normal range of the lymphocyte count is 1000 – 4800/µL. Their life span may vary from several days to a lifetime (as for memory lymphocytes). Unlike neutrophils, monocytes, and eosinophils, the lymphocytes 1) can move back and forth between the vessels and the extravascular tissues, 2) are capable of reverting to blast-like cells, and 3) when so transformed, can multiply as the immunologic need arises.
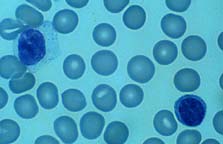
In normal people, most of lymphocytes are small, innocent-looking round cells with heavily “painted-on” nuclear chromatin, scant watery cytoplasm, and no granules. A small proportion of normal lymphs are larger and have more opaque, “busy-looking” cytoplasm and slightly irregular nuclei. Some of these have a few large, dark blue granules, the so called “azurophilic granules.” It has been maintained that these granulated cells are T-gamma cells (i.e., T-cells that have a surface receptor for the IgG Fc region) or natural killer (NK) null-cells. Other phenotypes of lymphocytes are not recognizable as such on the routine, Wright-stained smear and require special techniques for identification.
When activated by whatever means, lymphocytes can become very large (approaching or exceeding the diameter of monocytes) and basophilic (reflecting the increased amount of synthesized cytoplasmic RNA and protein). The cytoplasm becomes finely granular (reflecting increased numbers of organelles), and the nuclear chromatin becomes less clumped (the better to transcribe you with, my dear!). Such cells are called “transformed lymphocytes,” “atypical lymphocytes,” or “viral lymphocytes” by various votaries of blood smears. Although such cells are classically associated with viral infection (particularly infectious mononucleosis), they may also be seen in bacterial and other infections and in allergic conditions. A morphologic pitfall is mistaking them for monocytes (a harmless mistake) or leukemic blasts (not so harmless).


