
RBC (Red Blood Cell) Count
Share
Follow Us
The RBC count is most useful as raw data for calculation of the erythrocyte indices MCV and MCH .
Decreased RBC is usually seen in anemia of any cause with the possible exception of thalassemia minor, where a mild or borderline anemia is seen with a high or borderline-high RBC.
Increased RBC is seen in erythrocytotic states, whether absolute (polycythemia vera, erythrocytosis of chronic hypoxia) or relative (dehydration, stress polycthemia), and in thalassemia minor.
About Erythrocytes:
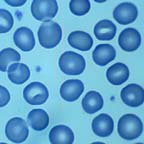
Structurally the simplest cell in the body, volumes have been written about the lowly red blood cell. The basic function of the rbc is the creation and maintenance of an environment salutary to the physical integrity and functionality of hemoglobin. In the normal state, erythrocytes are produced only in the skeleton (in adults only in the axial skeleton), but in pathologic states (especially myelofibrosis, which will be covered subsequently) almost any organ can become the site of erythropoiesis. Numerous substances are necessary for creation of erythrocytes, including metals (iron, cobalt, manganese), vitamins (B12, B6, C, E, folate, riboflavin, pantothenic acid, thiamin), and amino acids. Regulatory substances necessary for normal erythropoiesis include erythropoietin, thyroid hormones, and androgens. Erythrocytes progress from blast precursors in the marrow over a period of five days. Then they are released into the blood as reticulocytes, distinguishable from regular erythrocytes only with special supravital stains. The reticulocyte changes to an erythrocyte in one day and circulates for 120 days before being destroyed in the reticuloendothelial system.
Clinical laboratories measure several important parameters that reflect rbc structure and function. These measurements are used to 1) evaluate the adequacy of oxygen delivery to the tissues, at least as is related to hematologic (as opposed to cardiopulmonary) factors, and 2) detect abnormalities in rbc size and shape that may provide clues to the diagnosis of a variety of hematologic conditions. Most of these tests are performed using automated equipment to analyze a simple venipuncture sample collected in a universal lavender- (or purple-) top tube containing EDTA as an anticoagulant. Let us consider each of these tests.
- A. Hemoglobin concentration in whole bloodReferred to simply as “hemoglobin,” this test involves lysing the erythrocytes, thus producing an evenly distributed solution of hemoglobin in the sample. The hemoglobin is chemically converted mole-for-mole to the more stable and easily measured cyanmethemoglobin, which is a colored compound that can be measured colorimetrically, its concentration being calculated from its amount of light absorption using Beer’s Law. The normal range for hemoglobin is highly age- and sex-dependent, with men having higher values than women, and adults having higher values than children (except neonates, which have the highest values of all). For a typical clinical lab, the young adult female normal range is 12 – 16 g/dL; for adult males it is 14 – 18 g/dL.This is an easy test to perform, as hemoglobin is present in the blood in higher concentration than that of any other measured substance in laboratory medicine. The result is traditionally expressed as unit mass per volume, specifically grams per deciliter (g/dL). Ideologues in lab medicine have been maintaining for years that this unit will be replaced by Système Internationale (SI) units of moles per liter, but this has not gained any significant acceptance in clinical medicine except in the most nerdly circles.
- B. Erythrocyte countAlso referred to as just “rbc,” this simply involves counting the number of rbcs per unit volume of whole blood. Manual methods using the hated hemocytometer have been universally replaced by automated counting. The major source of error in the rbc count is an artificially reduced result that occurs in some conditions where rbcs stick together in the sample tube, with two or more cells being counted as one. The result of the test is expressed as number of cells per unit volume, specifically cells/µL. A typical lab’s normal range is 4.2 – 5.4 x 106/µL for females; for adult males it is 4.7 – 6.1 x 106 /µL.
- C. HematocritThis is also called the packed cell volume or PCV. It is a measure of the total volume of the erythrocytes relative to the total volume of whole blood in a sample. The result is expressed as a proportion, either unitless (e.g., 0.42) or with volume units (e.g., 0.42 L/L, or 42 cL/L [centiliters/liter]). An archaic way of expressing hematocrit is “volumes per cent” or just “percent” (42%, in the above illustration). Small office labs and stat labs measure hematocrit simply by spinning down a whole blood sample in a capillary tube and measuring the length of the column of rbcs relative to the length of the column of the whole specimen. Larger labs use automated methods that actually measure the volume individually of each of thousands of red cells in a measured volume of whole blood and add them up. The volume of individual erythrocytes can be electronically determined by measurement of their electrical impedance or their light-scattering properties. The normal range is 0.37 – 0.47 L/L for females, and 0.42 – 0.52 L/L for males.
- D. Erythrocyte indicesThe three cardinal rbc measurements described above (hemoglobin, hematocrit, and rbc count) are used to arithmetically derive the erythrocyte indices – mean corpuscular volume, mean corpuscular hemoglobin, and mean corpuscular hemoglobin concentration. As much as we all hate memorization, it is important to know how to calculate these indices and have some idea of the normal ranges. We will consider these individually.


