
Monocytes
Share
Follow Us
Monocytosis is seen in the recovery phase of many acute infections. It is also seen in diseases characterized by chronic granulomatous inflammation (TB, syphilis, brucellosis, Crohn’s disease, and sarcoidosis), ulcerative colitis, systemic lupus, rheumatoid arthritis, polyarteritis nodosa, and many hematologic neoplasms. Poisoning by carbon disulfide, phosphorus, and tetrachloroethane, as well as administration of griseofulvin, haloperidol, and methsuximide, may cause monocytosis.
Monocytopenia is generally not a clinical problem.
About Monocytes:
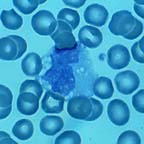
These large cells are actually more closely related to neutrophils than are the other “granulocytes,” the basophil and eosinophil. Monocytes and neutrophils share the same stem cell. Monocytes are to histiocytes (or macrophages) what Bruce Wayne is to Batman. They are produced by the marrow, circulate for five to eight days, and then enter the tissues where they are mysteriously transformed into histiocytes. Here they serve as the welcome wagon for any outside invaders and are capable of “processing” foreign antigens and “presenting” them to the immunocompetent lymphocytes. They are also capable of the more brutal activity of phagocytosis. Unlike neutrophils, histiocytes can usually survive the phagocytosis of microbes. What they trade off is killing power. For instance, mycobacteria can live in histiocytes (following phagocytosis) for years.
The normal range for the monocyte count is 200 – 950 /µL.


