
3 Methods to Predict Who Will Develop Liver Cancer After HCV Treatment
Share
Follow Us
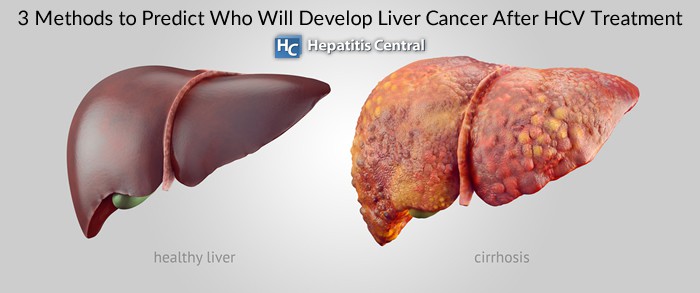

Hepatitis means the liver is inflamed in response to a virus. Hepatitis C in particular can range from a short-term infection that lasts a few weeks to a serious, long-term illness. When hepatitis C becomes chronic (meaning long-term), it can result in serious complications including liver damage, liver failure, cirrhosis, and liver cancer. (1)
A set of studies presented at the Digital International Liver Congress the end of August 2020 found three new methods to predict who will develop liver cancer after successful treatment of the hepatitis C virus.
Hepatitis Symptoms and Risk
At this time vaccines are available for hepatitis A and B, but not hepatitis C. Symptoms often don’t show themselves when an individual is infected, which is why it is deemed as the “silent” infection.
When the virus lingers long enough to damage the liver, symptoms will arise such as: (2)
- Bleeding and bruising easily
- Fatigue
- Poor appetite
- Yellow discolorations of the skin and eyes (jaundice)
- Fluid buildup in abdomen (ascites)
- Confusion, drowsiness, and slurred speech (Hepatic encephalopathy)
For an unclear reason, individuals born between 1945 and 1965 (AKA baby boomers) have at least 5 times the risk of having hepatitis C compared to people in other age groups.
Additional risk factors include: (3)
- Exposure to the virus through IV drug use
- Long-term hemodialysis
- Organ transplant or blood transfusion prior to 1992
- HIV diagnosis
- Exposure to infected blood by a needle
- Receiving clotting factor concentrates produced before 1987
- Children born to hepatitis C-positive women
- Piercing or tattoo with unsterile equipment
About 30% of individuals who are exposed to hepatitis C will clear the virus on their own, but that leaves an additional 70% who will go on to have chronic hepatitis. (3) As we had already mentioned, chronic hepatitis leads to liver complications which could ultimately turn into cancer.
Hepatocellular carcinoma (HCC) is the most common form of liver cancer that can occur due to chronic hepatitis C. Individuals who are cured of hepatitis C are less likely to develop HCC, but there is still a possibility especially with the development of cirrhosis.
A late diagnosis of HCC brings about challenges when it comes to treatment, therefore finding methods to predict who is at greater risk of developing liver cancer is needed.
Study #1
Jessica Azzi, PharmD, of the ANRS-AFEF HEPATHER Study Group located in Paris along with her colleagues analyzed factors and created a prognostic score for HCC after sustained virological response (SVR, means hepatitis C has not been detected in the blood 12 weeks or more after completing treatment) to direct-acting antiviral (DAA) therapy. (4)
The analysis included 3,929 individuals who were diagnosed with chronic hepatitis C and were cured with DAAs. 2,829 people had cirrhosis, with 191 (approximately 6.8%) developing liver cancer. On the other hand, 15 of 1,097 people (1.4%) with moderate to advanced fibrosis developed HCC.
The researchers found 11 different variables associated with HCC, including:
- Male sex
- Age greater than 64
- Hepatitis C virus genotype 3 (higher rate of steatosis and fibrosis progression)
- Prolonged prothrombin time (a measure of blood clotting ability)
- Alpha-fetoprotein (AFP, a liver cancer biomarker)
- FIB-4 score (fibrosis index based on lab tests)
- High cholesterol
- Esophageal varices (enlarged veins)
- Prior treatment with interferon-based therapy
- Span of hepatitis C infection
- Underweight
Each of these variables were assigned points which were then tallied up to create an HCC risk score. Here is what the scores mean:
- Below 6 = low risk
- 6 to 11 = medium risk
- 11 or above = high risk
After a 3-year follow up, only 2% with low risk developed HCC, 7% at medium risk, and 23% who were high risk.
This tool is a simple way to estimate risk of HCC and can also be cost effective for individuals seeking liver cancer screening.
Study #2
Pierre Nahon, MD, PhD, of Jean Verdier Hospital in Paris along with his colleagues wanted to identify commonly measured biomarkers and changes in AFP levels (the liver cancer biomarker) that could potentially predict the risk of HCC in individuals with cirrhosis. (4)
This study was a bit smaller with 717 participants who were followed for around 5.6 years, with 413 individuals achieving SVR. The lab levels that were assessed every 6 months included:
- Liver enzymes (ALT, AST, and GGT)
- Bilirubin
- AFP
- Albumin
- Platelets
- Prothrombin
Before SVR, the researchers determined three groups:
- People with inflammation and high AFP levels (highest risk of developing HCC)
- Those who experienced liver failure (high risk of developing HCC)
- Those with the least impaired lab values (lower risk of developing HCC)
When individuals achieved SVR, they were grouped like this:
- Persistent liver impairment
- Continued to have elevated liver biomarkers
- Least impaired values
From these groups, the individuals who were dealing with persistent liver impairment and/or elevated biomarkers were at higher risk of developing HCC whereas least impaired value group had a low rate. Researcher Nahon believed that the individuals dealing with persistent liver impairment even after being cured of hepatitis were treated too late.
The conclusion was that pre-SVR inflammation and liver failure clusters represented two different risk profiles that accounted for more than half of individuals who developed liver cancer. Even after SVR, these profiles can continue and identify groups who are still at risk for HCC.
Study #3
Gamal Shiha, MD, PhD, of the Egyptian Liver Research Institute and Hospital near Cairo worked with his colleagues to develop a non-invasive scoring model for HCC risk prediction. (4)
After over 200,000 people were screened for hepatitis C in Egypt (and treating those with the infection), researchers identified 2,372 people without existing liver cancer who had achieved SVR and completed a year of follow up. Of those people, nearly ¾ had cirrhosis and the rest had advanced fibrosis.
After 2 years of follow-up, 109 individuals developed HCC after the end of their treatment. Everyone except 8 people had cirrhosis before starting their hepatitis C treatment.
Risk factors for developing liver cancer included:
- Older age (over 54)
- Male sex
- Pretreatment fibrosis stage (cirrhosis vs. advanced cirrhosis)
- AFP
- Albumin levels
A score was then created by assigning points to each variable. Three groups were created:
- Low risk = a score of 6 or lower
- Intermediate risk = score of 6 to 7.5
- High risk = score of 7.5 or over
The score proved high predictive accuracy, with HCC incidence rates of:
- 1.2% for low risk group
- 3.3% for intermediate risk group
- 7.1% for high risk group
Other cohorts who tested the score theory also showed that it was accurate. One cohort of 947 patients with cirrhosis and 394 with advanced fibrosis showed:
- 1 person in the low risk group developed HCC
- 6 people in the intermediate group developed HCC
- 39 people in the high risk group developed HCC
Shiha suggested that this will help to identify individuals who would benefit from continued HCC surveillance and allow those at highest risk to enable a personalized surveillance strategy.
Related Articles

- Hepatitis C Questions and Answers for the Public. (2020, July 28). Retrieved October 01, 2020, from https://www.cdc.gov/hepatitis/hcv/cfaq.htm
- Hepatitis C. (2020, March 20). Retrieved October 01, 2020, from https://www.mayoclinic.org/diseases-conditions/hepatitis-c/symptoms-causes/syc-20354278
- MD Anderson Cancer Center, & Underferth, D. (2019, May 08). Hepatitis C and liver cancer: What to know. Retrieved October 01, 2020, from https://www.mdanderson.org/publications/focused-on-health/HepatitisC-liver-cancer-What-you-need-to-know.h16Z1591413.html
- Predicting Liver Cancer in People Cured of Hepatitis C. (2020, September 20). Retrieved October 01, 2020, from https://www.hepmag.com/article/predicting-liver-cancer-people-cured-hepatitisC


